2 Greenwich Office Park
Suite 210
Greenwich, CT 06831
203 863-0003
77 Lafayette Place
Suite 302
Greenwich, CT 06830
203 863-0003
21 Reade Place
Suite 2100
Poughkeepsie, NY 12601
203 863-0003
© 2024 The Plastic & Reconstructive Surgery Group - All Rights Reserved - Featured Realself Breast Reconstruction Expert - Terms of Use - Sitemap
The Thigh As A Donor Site: PAP, DUG and TUG Flaps
Menu

PAP Flap, DUG Flap and TUG Flap
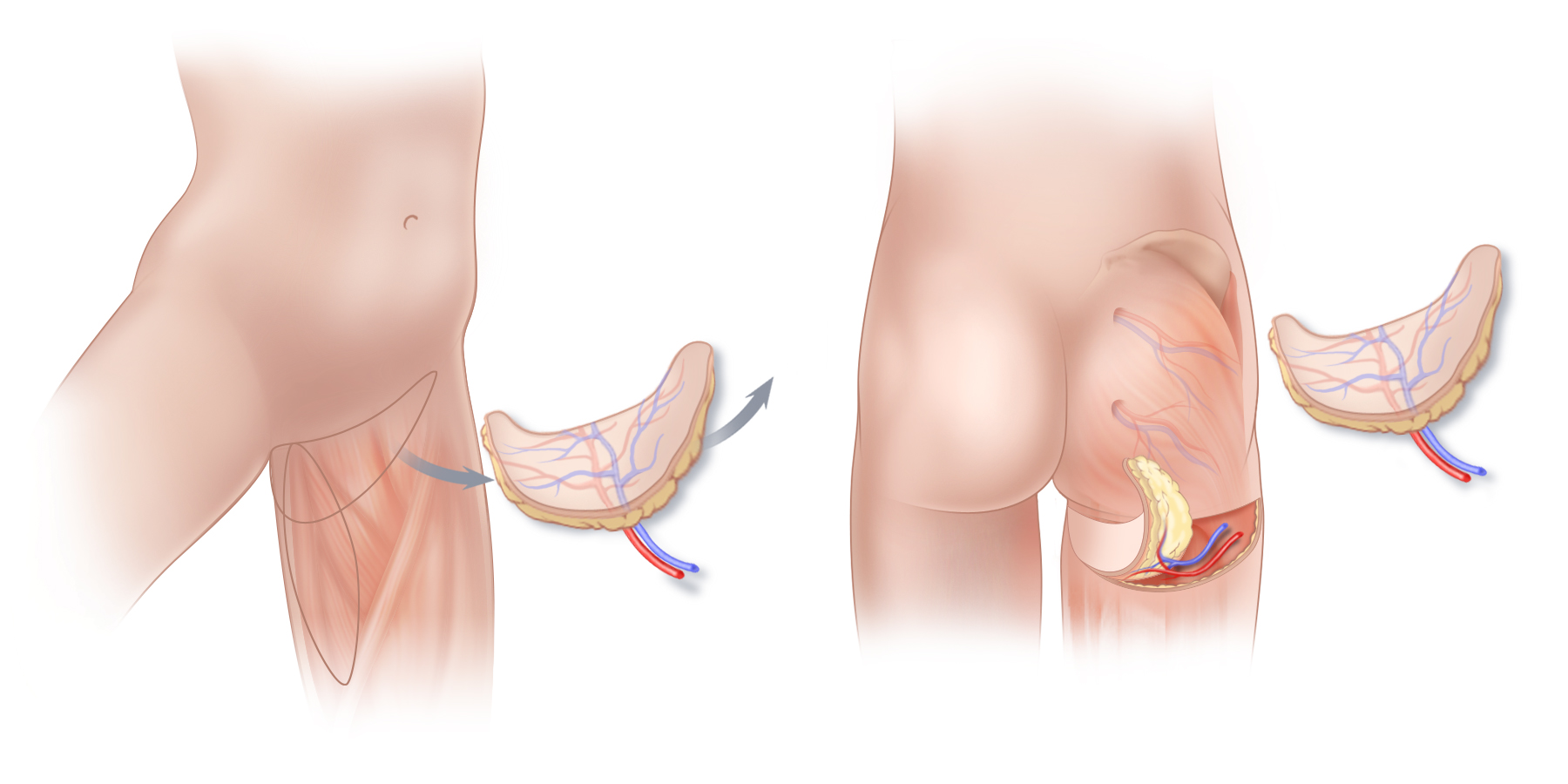
Tissue from the upper thigh can be used for natural-tissue breast reconstruction. (A) the Transverse Upper Gracilis or TUG flap, and the Diagonal Upper Gracilis or DUG flap may be good options when excess tissue is present on the inner thigh. Although technically TUG and DUG flaps are not perforator flaps, TUG/DUG flaps remove only a small piece of muscle from the inner thigh, an area of the body with a very large muscle mass, and thus weakness and functional impairment are avoided. (B) Tissue from the back of the upper thigh (PAP Flap) can also be used for natural-tissue breast reconstruction. The scar that results following a PAP flap procedure will vary from person to person as the anatomy of the blood vessels in this portion of the thigh is quite variable.
Tissue from the upper thigh can be used for natural-tissue breast reconstruction. (A) the Transverse Upper Gracilis or TUG flap, and the Diagonal Upper Gracilis or DUG flap may be good options when excess tissue is present on the inner thigh. Although technically TUG and DUG flaps are not perforator flaps, TUG/DUG flaps remove only a small piece of muscle from the inner thigh, an area of the body with a very large muscle mass, and thus weakness and functional impairment are avoided. (B) Tissue from the back of the upper thigh (PAP Flap) can also be used for natural-tissue breast reconstruction. The scar that results following a PAP flap procedure will vary from person to person as the anatomy of the blood vessels in this portion of the thigh is quite variable.
The skin and fat of the upper thigh can be used to reconstruct breasts with a natural appearance using warm, supple, living tissue. The Profunda Artery Perforator flap or PAP flap, the Transverse Upper Gracilis or TUG flap, and the Diagonal Upper Gracilis or DUG flap can be good options for breast reconstruction for some women. The shape of these flaps facilitates the sculpting of breasts with especially youthful projection and contour. However, because PAP flaps, DUG flaps, and TUG flaps generally produce a scar on the upper thigh that is not well-hidden by a bathing suit, and because these flaps can sometimes result in a change in thigh and lower buttock contour that is unfavorable, PAP, DUG and TUG flaps are generally used in our practice, only when other, more favorable donor sites are not an option.
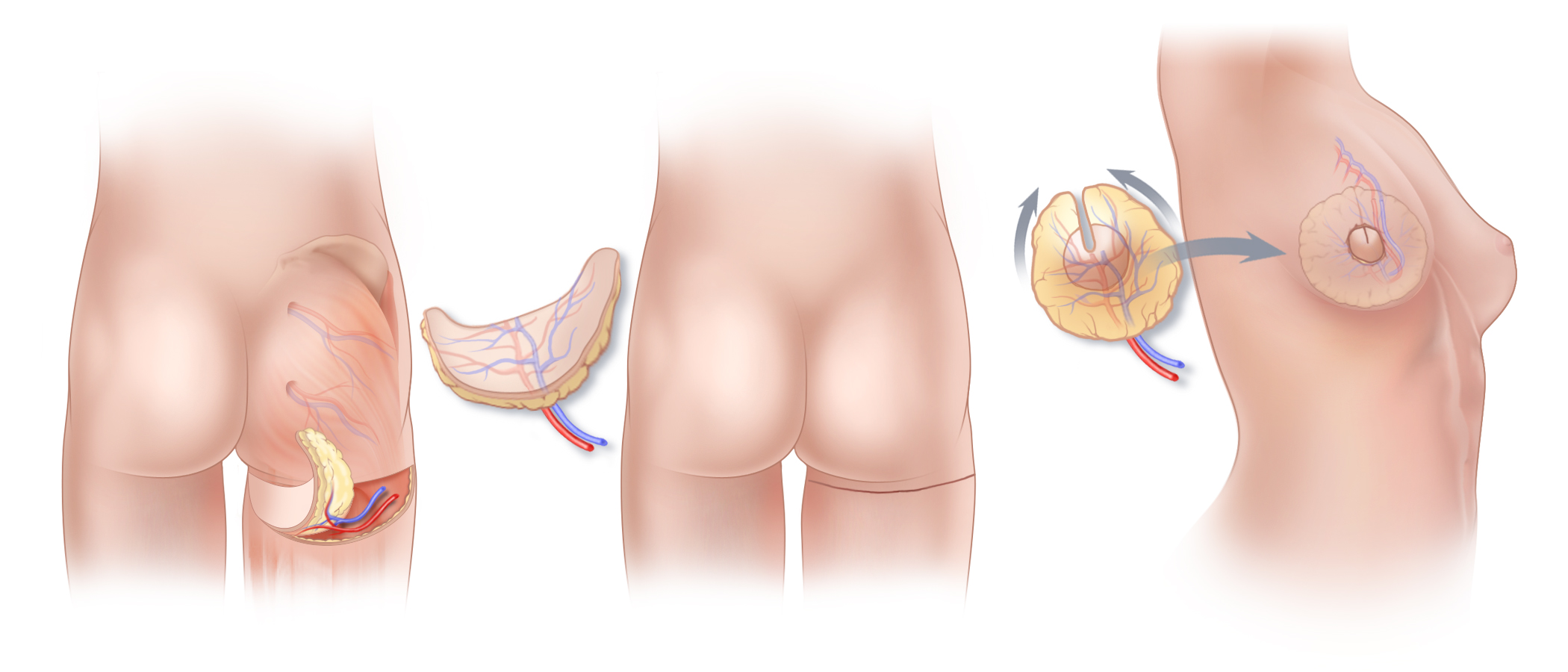
Tissue from the upper part of the thigh can be used for natural-tissue breast reconstruction. (B) The scar that results following a PAP flap procedure lies on the back of the thigh, ideally just below the lower buttock crease, but often lower down. The scar typically extends somewhat onto both the inner and outer thighs. (C) Similar to the way in which TUG and DUG flaps are shaped to reconstruct a breast, by bringing the ends of the PAP flap together, the crescent-shaped flap is formed into a reconstructed breast with youthful contours and projection. The flap is transferred to the chest, and the blood vessels of the PAP flap are connected to blood vessels at the chest using microsurgical techniques. The location of the surgical scar on the breast will depend on the technique used for the mastectomy itself.
Tissue from the upper part of the thigh can be used for natural-tissue breast reconstruction. (B) The scar that results following a PAP flap procedure lies on the back of the thigh, ideally just below the lower buttock crease, but often lower down. The scar typically extends somewhat onto both the inner and outer thighs. (C) Similar to the way in which TUG and DUG flaps are shaped to reconstruct a breast, by bringing the ends of the PAP flap together, the crescent-shaped flap is formed into a reconstructed breast with youthful contours and projection. The flap is transferred to the chest, and the blood vessels of the PAP flap are connected to blood vessels at the chest using microsurgical techniques. The location of the surgical scar on the breast will depend on the technique used for the mastectomy itself.
The PAP, TUG and DUG flaps are similar to one another, in that they all come from the upper thigh. The technique and resultant scar vary from one flap to another, and the distribution of fatty tissue on an individual’s upper thigh will play a role in determining which of these flaps is best suited for her. The PAP flap uses tissue from the back of the thigh, whereas the TUG and DUG flaps take tissue from the inner thigh. While the PAP flap is a true perforator flap, and therefore does not take any muscle from the donor site, DUG and TUG flaps require that a small amount of gracilis muscle be incorporated into the flap to assure the adequacy of blood flow. However, since the gracilis muscle is a very small muscle (unlike the rectus abdominis muscle on the abdomen), and not one of the primary muscles of the leg, it is generally not missed after TUG or DUG flap breast reconstruction surgery, and there is no risk of developing a hernia at the donor site.
TUG Flap, PAP Flap and DUG Flap Surgery in Connecticut and New York
Please Contact us if you would like more information about TUG flap, DUG flap or PAP flap breast reconstruction, or information about other options for breast reconstruction including DIEP flap surgery after mastectomy. Our practice has offices in New York and Greenwich, Connecticut.